Deck 10: Recording Skills: the Basis for Data Collection, Organization,
Full screen (f)
Question

Unlock Deck
Sign up to unlock the cards in this deck!
Unlock Deck
Unlock Deck
1/1
Play
Full screen (f)
Deck 10: Recording Skills: the Basis for Data Collection, Organization,
Study #1 (Pleural Effusion)
Admitting History and Physical Examination
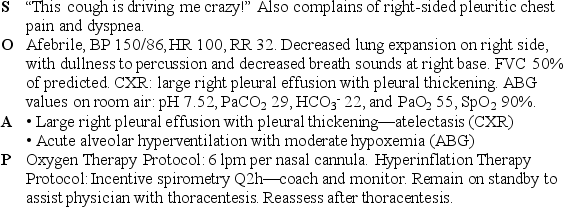
A 55-year-old man came to the emergency department because of dull, right-sided chest pain of about 2 weeks' duration; dry, nonproductive cough; and increasing dyspnea. He had a history of having worked with asbestos insulating materials for about 1 month almost 30 years previously. The patient had never smoked.
On physical examination the patient appeared older than his stated age and was in obvious, moderately severe respiratory distress. His oral temperature was 98.6° F; blood pressure was 150/86, pulse 100/min, and respirations 32/min. Examination of the chest showed decreased respiratory excursion on the right side, with dullness to percussion and diminished breath sounds in this area. No wheezes or rhonchi were heard.
Bedside spirometry revealed an FVC that was 50% of predicted. The chest radiograph revealed a large pleural effusion, lung atelectasis, and pleural thickening in the lower right lung area. Room air blood gases were pH 7.52, PaCO2 29, HCO3- 22, and PaO2 55. His WBC was 10,400. His oxygen saturation was 90%. The physician prepared the patient for a thoracentesis. Complete a SOAP for the patient at this time.
Admitting History and Physical Examination
A 55-year-old man came to the emergency department because of dull, right-sided chest pain of about 2 weeks' duration; dry, nonproductive cough; and increasing dyspnea. He had a history of having worked with asbestos insulating materials for about 1 month almost 30 years previously. The patient had never smoked.
On physical examination the patient appeared older than his stated age and was in obvious, moderately severe respiratory distress. His oral temperature was 98.6° F; blood pressure was 150/86, pulse 100/min, and respirations 32/min. Examination of the chest showed decreased respiratory excursion on the right side, with dullness to percussion and diminished breath sounds in this area. No wheezes or rhonchi were heard.
Bedside spirometry revealed an FVC that was 50% of predicted. The chest radiograph revealed a large pleural effusion, lung atelectasis, and pleural thickening in the lower right lung area. Room air blood gases were pH 7.52, PaCO2 29, HCO3- 22, and PaO2 55. His WBC was 10,400. His oxygen saturation was 90%. The physician prepared the patient for a thoracentesis. Complete a SOAP for the patient at this time.
(suggested):
Respiratory Assessment and Plan
 Discussion
Discussion
The respiratory care practitioner's involvement in the care of patients with pleural disease/pleural effusion is often somewhat limited. The patient's hypoxemia and secondary alveolar hyperventilation reflect his lung compression atelectasis (see Figure 9-7). Hyperinflation therapy was clearly indicated after the chest X-ray showed a large right pleural effusion (see Protocol 9-3). Oxygen therapy per protocol was indicated because of the patient's hypoxemia (see Protocol 9-1).
Respiratory Assessment and Plan
DiscussionThe respiratory care practitioner's involvement in the care of patients with pleural disease/pleural effusion is often somewhat limited. The patient's hypoxemia and secondary alveolar hyperventilation reflect his lung compression atelectasis (see Figure 9-7). Hyperinflation therapy was clearly indicated after the chest X-ray showed a large right pleural effusion (see Protocol 9-3). Oxygen therapy per protocol was indicated because of the patient's hypoxemia (see Protocol 9-1).
Unlock Deck
Unlock for access to all 1 flashcards in this deck.



