Global Business 4th Edition by Mike Peng
Edition 4ISBN: 978-1305500891Global Business 4th Edition by Mike Peng
Edition 4ISBN: 978-1305500891 Exercise 24
Farmacias Similares: Innovating in the Mexican Healthcare Industry1
Miguel A. Montoya (Tecnologico de Monterrey)
Mauricio Cervantes (Tecnologico de Monterrey)
In the Mexican healthcare industry, Best Laboratories created Farmacias Similares (FS) in 1997 with a new Pharmacy- Doctor business model, which started by focusing on the base of the pyramid (BoP). The successful model recently penetrated higher-income markets in Mexico as well. Looking forward, the Board needs to decide which direction to focus on.
The Board of Farmacias Similares wants to maintain the firm growth rate of the past few years. Next month it will have its annual meeting and need to make a very strategic decision: should the firm migrate to focus on the low-income class in other Latin American countries or should it migrate to focus on the high-income class in Mexico.
Introduction
For over four decades, Best Laboratories, a Mexicanowned company founded in 1953, concentrated exclusively on the production and supply of generic drugs for Mexican public health institutions. This model had a significant weakness: a single client the government, a lot of competition, and low profit margins (see Appendix 1). Faced with these challenges, in 1997 Best Laboratories saw a huge opportunity with a change in the law allowing the sale of generic medicine directly to the public.2 At first Best Laboratories tried to sell the generic drugs through private pharmacy chains. However, due to a campaign to discredit generic medicine, existing private pharmacy chains in Mexico refused to sell the generic drugs. As a result the current distribution channels were of no use to Best Laboratories. This situation motivated Best Laboratories to create its own distribution channels in order to fulfil the needs of the base of the pyramid (BoP), by offering cheap generic drugs in direct contrast to the expensive brand-name drugs sold by the current private pharmacy chains. However, the majority of private doctors continued to prescribe brand-name drugs. The excess of medical professionals, low profits, and refusal of the private network to use generic drugs-combined with the fact that there was only a single client and that there was a large amount of the population without access to medical services-pushed Best Laboratories to create Farmacias Similares (FS) in 1997 with a new Pharmacy- Doctor business model.
FS began with one pilot model in 1997, which increased to two in 1998. There was then a large increase to 144 in 1999. The initial objective was to supply generic medicines to the BoP population without access to public health insurance (59% in 1997), mainly covering those working in the informal economy who lacked public health insurance and who could not afford private healthcare. At that time the Mexican population was growing at 2% annually, with the urban BoP population also continuing to expand, signifying an expanding market for the new service. The FS model is comprised of a small medical clinic attached to the pharmacy where clients visit the doctor for a nominal fee (no more than US$2) and receive a quick prescription. The consumer then purchases the generic drugs quickly and cheaply at the FS pharmacy, with most drugs being 50% cheaper than their brand-name equivalents. The FS medical service is available for over 12 hours daily. Right from the start, users interviewed reported that the convenient location of the pharmacies, the low-cost medical service, and the lack of the requirement for an appointment-together with the availability of generic medicine at affordable prices-made FS one of the best options for the treatment of illnesses not requiring hospitalization.
Increasing Market Share in the Low-Cost Segment
Competitors of FS (mostly multinational drug makers) criticized the quality of the generic drugs sold by FS. But a series of tests carried out by the authorities, as well as universities and multinational laboratories, showed that FS drugs were reliable. The innovative low-cost Pharmacy-Doctor model enjoyed rapid growth within the BoP in Mexico: in 1998 the company had two instore medical clinics, a number that expanded to 1,215 in 2003, 3,630 in 2008, and 4,053 in 2011. More than 5 million visits a month were recorded in 2011, with the cost of the medical consultation being approximately US$2. FS only sold generic drugs, and over 220 million generic units were sold in 2013, achieving a market penetration of 60% of units sold. The Pharmacy-Doctor business model immediately began to spread within the industry. GI Pharmacies began operations in 1999, simultaneously piloting the low-cost Pharmacy-Doctor model for the BoP population and purchasing generic drugs from several laboratories. GI is only a distributor: it has no dedicated laboratories and 110 plans to integrate the entire process in the same manner as FS.
The successful Pharmacy-Doctor business model for those lacking health insurance pioneered by FS gradually became threatened by new legislation. At the beginning of 2003, the government launched the Seguro Popular (universal public health insurance), offering medical coverage to all Mexicans with no formal employment and therefore without access to IMSS or ISSSTE. Seguro Popular coverage grew rapidly, and by 2011 more than 49 million Mexicans were affiliated (43% of the population). As a result, when adding 52 million Social Security system users and users of other public health systems, the country's public health coverage reached over 89% of the population. The market segment of the BoP for FS was therefore reduced from 59% in 1997 to 11% in 2011. As the innovation grew in acceptance, an unforeseen factor came into play: the ability of the system to save service-users time. Although IMSS, ISSSTE, and Seguro Popular are totally free, they have a long waiting list for their services, including emergencies. The BoP population is mostly employed in the informal sector, meaning if people lose time waiting for medical services they lose their daily wage. It is also difficult for employees to obtain permission to visit the doctor's office. BoP clients prefer to spend an average between US$7 and US$10 on a doctor's prescription and medicine than to lose their daily wage waiting in line for free public services.
Despite the increase in public health coverage, the new Pharmacy-Doctor model continued to grow. The perception of poor quality of public health services (such as significant waiting time before being seen by a doctor and a lack of medicine in public health institutions) provided an opportunity for the consolidation of the new model. An interview with a lower middleclass user of state-run medical services revealed that: "even with an advance appointment, the waiting time for a consultation is about three hours." The interviewee further stated that visiting the doctor with no appointment involved an average wait of more than five hours, despite the average consultation not exceeding ten minutes. Finally, the interviewee claimed that "in most cases, four out of five, the drug is not free".
As the Pharmacy-Doctor model started to become more established, positive discussions on the quality of generic medicines and brand-name rights between FS and international drug makers began to take place, resulting in collaboration between the various actors. An example of this would be Sancloz de Mexico, the generic division of the Novartis Group, which began to work towards becoming the supplier for FS. Regardless of the efficiency of implementation and the increasing healthcare coverage resulting from Seguro Popular, the FS Pharmacy-Doctor model continued to grow. The emergence of the model and its nationwide diffusion in the BoP by FS was a huge success.
Imitators in the High-lncome Level Segment
Up until 2011, FS and GI focused on servicing the BoP and had no plans to enter the healthcare field for the middle or upper class in Mexico. In 2009, external events once again affected the dynamics of the model. Mexico was affected by a pandemic (the H1N1 influenza virus), leading to increased regulations of drug sales and making a prescription mandatory for the sale of antibiotics. This became a strong contributing factor to the diffusion of the business model. The treatment of H1N1 was complicated because the Mexican population was accustomed to selfLmedication without the necessity of a prescription. The lack of national regulations preventing the sale of antibiotics without a prescription and the prevalence of self-medication led to the deaths of several people affected by H1N1. In order to address this problem, in May 2010 the government tightened the regulations governing the sale of drugs, particularly the sale of antibiotics. These legislative changes, combined with an ever-increasing time-poor middle and upper classes, helped the Pharmacy-Doctor model to diffuse to large segments of the population.
In 2011, the majority of the national pharmacy chains had adopted the Pharmacy-Doctor model in most of their branches, not just in areas populated by the BoP, but also in mainly middle and upper-class neighborhoods. Initially pharmacies sold brand-name drugs. But by 2011, many adopted the new model, making space within the pharmacy for a doctor's office. Today many pharmacies offer an almost identical model: a physician who can be seen quickly (10 to 15 minutes waiting time) and economically (up to US$2.50 per consultation), attached to a pharmacy offering brand-name (normallypriced) drugs and generic (economically-priced) drugs.
Therefore, the model initially conceived for the BoP in effect migrated upwards to serve middle and upper-income market segments, a process described as trickle-up innovation. Just as with the BoP, the middle and upper classes also go to the pharmacy to consult a doctor in order to treat symptoms not requiring hospitalization. They are able to purchase not only generic drugs, but also brand-name drugs.
The great difference between the BoP and the middle and upper-classes is in the reason why they go to the new Pharmacy-Doctor clinics: the latter group has access to public medical services as well as private insurance (the majority have both) and can easily afford to pay the fees charged by private doctors. The main reason both groups use the service is that they are short on time. Time is extremely valuable for urban populations in general, and the quick service has become the main success factor in the new model. In addition, the requirement for a medical prescription, the proximity of the service to the patient's home and work, and low prices are the main contributory factors behind their decision to use the service.
The middle and upper classes believe that significant time is wasted in waiting to obtain private appointments, and that such appointments, once obtained, are liable to significant delay. In addition, they frequently cost up to US$50 or more. Private health insurance in the country generally has a high deductible, usually more than US$300, and so is not used for common or minor ailments. Pharmacies located in middle or upper-class neighborhoods are spacious, comfortable (with parking and air conditioning) with a large range of medicines and related items. The first pharmacies to offer an onsite medical consultation service, FS, were small stores, with the doctor's office immediately adjacent to the pharmacy, being separated from it by a thin wall. Doctor's offices in Farmacias Guadalajara or Del Ahorro are generally larger in size overall and always have a street-door. In supermarkets such as Walmart the consulting room is usually located inside the store and always next to the pharmacy (see Exhibit 1).
In the beginning, the legislative change making drug prescriptions mandatory negatively affected sales of medicines in drugstores that did not offer low-cost physician consultations. This in turn led to pharmacy chains for all social strata (BoP, middle class, and upper class) seeking to implement the Pharmacy- Doctor business model. As a result, the model diffused upwards socially bringing the Pharmacy-Doctor pairing to middle and upper-class clients. Consumers are willing to pay out-of-pocket for Pharmacy-Doctor clinics to receive care more quickly. Many are willing to use a Pharmacy-Doctor clinic for a minor condition if it means being seen immediately. Pharmacy chains that offer their products to wealthy social classes have thus adopted a model originally designed for the BoP, realizing that there is an opportunity to increase sales due to the fact that even the middle or upper classes do not go to their private doctor for a prescription for minor ailments. As one FS patient commented: "The wait was 10 minutes and the consultation was 15 minutes. The doctor's professional qualification was from a highlyregarded private school in the area. The attention was good and I paid US$1.5 for the consultation and US$2 for the medicine. My eye infection disappeared in two days." Doctors consulting inside the pharmacies also viewed this avenue as a useful way of obtaining experience after graduation and helping them to decide on a future specialization.
Overall, the new Pharmacy-Doctor model is a winwin- win for consumers (patients), drug makers, and doctors. It is a successful innovation that has proliferated throughout the Mexican healthcare industry (Exhibit 2). Looking forward, the Board of Farmacias Similares, which pioneered this model, needs to make a strategic decision: should the firm go international and export the model to focus on the low-income class in other Latin American countries or should it stay domestic and further penetrate the higher-income (middle and upper-class) markets in Mexico.
Appendix 1. The Healthcare Industry in Mexico In 1997 the healthcare industry was mainly made up of the following: the Mexican Public Health Service (IMSS) founded in 1943 and covering 35% of the population; the Government Workers Social Security Scheme (ISSSTE) founded in 1960 and covering 5% of the population; and other social security systems founded between 1940 and 1950 and covering 1% of the population. In 1997, Mexico had approximately 59% of the population without medical coverage, the majority of whom belonging to the BoP. In addition, there is a private network of insurance companies, hospitals, pharmacies, and doctors that charge expensive fees for their medical services and medicines. This private network is used by the middle and upper classes as they can afford to take out private health insurance, and this private network covers 19% of the population. This 19% is already covered by the IMSS or ISSSTE, since these individuals are most likely employees and all employers must provide public service benefits. However, this segment takes out private insurance in order to avail itself of the private network, which is believed to be more efficient than the IMSS or ISSSTE: only in extreme cases does this segment use the public service. The individuals who comprise of the BoP, who are excluded from public medical services and unable to afford the private services, generally have to use alternative medicines, such as homeopathy, herbal medicine, and traditional healers that arc the only options economically available to them.
The network of private pharmacies sells only brandname drugs manufactured by international drug makers, while public-sector pharmacies use mainly generic drugs manufactured by national and international drug makers. Since the IMSS has the widest population coverage, competition among companies to be official suppliers has resulted in allegations of widespread corruption. Another noteworthy characteristic of the medical industry is the excellent social status that doctors have, along with the excellent wages they can earn in private hospitals or consultancies. Annually more doctors graduate from Mexican universities than are required in large urban areas. There is a scarcity of doctors in rural areas, but the majority prefer urban to rural environments as low-income people are often unable to pay for medical services. As a result, many medical graduates swell the ranks of the urban underemployed, filling temporary positions. This is a general picture of the conditions prevailing in the medical
industry in Mexico in 1997.
1) © Miguel A. Montoya and Mauricio Cervantes. Reprinted with permission.
2) Generic medications are those sold under the name of the active ingredient, in contrast to brand-name drugs that are manufactured worldwide by different pharmaceutical companies for brand-name owners.
Sources: Extracted from (1) company web pages; (2) Euromonitor International, 2012, Consumer Health-Mexico, Retrieved February 12, 2012, www.euromonitor.com/mexico; (3) R Keckley, S. Coughlin, L. Korenda, G. Moreno, 2011, Survey of Health Care Consumers in Mexico: Key Findings, Strategic Implications, Deloitte Center for Health Solutions.
Exhibit 1 Examples of Pharmacy-Doctor Model Layouts

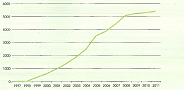
Exhibit 2 Growth of the pharmacy-Doctor Model in the Base of the Pyramid in Mexico, 1997-2011
Number of pharmacies of FS and GI combined.
From a resource-based view, how easy or difficult it is for competitors to offer a similar Pharmacy- Doctor business model? Given your answer, how sustainable is FS's competitive advantage?
Miguel A. Montoya (Tecnologico de Monterrey)
Mauricio Cervantes (Tecnologico de Monterrey)
In the Mexican healthcare industry, Best Laboratories created Farmacias Similares (FS) in 1997 with a new Pharmacy- Doctor business model, which started by focusing on the base of the pyramid (BoP). The successful model recently penetrated higher-income markets in Mexico as well. Looking forward, the Board needs to decide which direction to focus on.
The Board of Farmacias Similares wants to maintain the firm growth rate of the past few years. Next month it will have its annual meeting and need to make a very strategic decision: should the firm migrate to focus on the low-income class in other Latin American countries or should it migrate to focus on the high-income class in Mexico.
Introduction
For over four decades, Best Laboratories, a Mexicanowned company founded in 1953, concentrated exclusively on the production and supply of generic drugs for Mexican public health institutions. This model had a significant weakness: a single client the government, a lot of competition, and low profit margins (see Appendix 1). Faced with these challenges, in 1997 Best Laboratories saw a huge opportunity with a change in the law allowing the sale of generic medicine directly to the public.2 At first Best Laboratories tried to sell the generic drugs through private pharmacy chains. However, due to a campaign to discredit generic medicine, existing private pharmacy chains in Mexico refused to sell the generic drugs. As a result the current distribution channels were of no use to Best Laboratories. This situation motivated Best Laboratories to create its own distribution channels in order to fulfil the needs of the base of the pyramid (BoP), by offering cheap generic drugs in direct contrast to the expensive brand-name drugs sold by the current private pharmacy chains. However, the majority of private doctors continued to prescribe brand-name drugs. The excess of medical professionals, low profits, and refusal of the private network to use generic drugs-combined with the fact that there was only a single client and that there was a large amount of the population without access to medical services-pushed Best Laboratories to create Farmacias Similares (FS) in 1997 with a new Pharmacy- Doctor business model.
FS began with one pilot model in 1997, which increased to two in 1998. There was then a large increase to 144 in 1999. The initial objective was to supply generic medicines to the BoP population without access to public health insurance (59% in 1997), mainly covering those working in the informal economy who lacked public health insurance and who could not afford private healthcare. At that time the Mexican population was growing at 2% annually, with the urban BoP population also continuing to expand, signifying an expanding market for the new service. The FS model is comprised of a small medical clinic attached to the pharmacy where clients visit the doctor for a nominal fee (no more than US$2) and receive a quick prescription. The consumer then purchases the generic drugs quickly and cheaply at the FS pharmacy, with most drugs being 50% cheaper than their brand-name equivalents. The FS medical service is available for over 12 hours daily. Right from the start, users interviewed reported that the convenient location of the pharmacies, the low-cost medical service, and the lack of the requirement for an appointment-together with the availability of generic medicine at affordable prices-made FS one of the best options for the treatment of illnesses not requiring hospitalization.
Increasing Market Share in the Low-Cost Segment
Competitors of FS (mostly multinational drug makers) criticized the quality of the generic drugs sold by FS. But a series of tests carried out by the authorities, as well as universities and multinational laboratories, showed that FS drugs were reliable. The innovative low-cost Pharmacy-Doctor model enjoyed rapid growth within the BoP in Mexico: in 1998 the company had two instore medical clinics, a number that expanded to 1,215 in 2003, 3,630 in 2008, and 4,053 in 2011. More than 5 million visits a month were recorded in 2011, with the cost of the medical consultation being approximately US$2. FS only sold generic drugs, and over 220 million generic units were sold in 2013, achieving a market penetration of 60% of units sold. The Pharmacy-Doctor business model immediately began to spread within the industry. GI Pharmacies began operations in 1999, simultaneously piloting the low-cost Pharmacy-Doctor model for the BoP population and purchasing generic drugs from several laboratories. GI is only a distributor: it has no dedicated laboratories and 110 plans to integrate the entire process in the same manner as FS.
The successful Pharmacy-Doctor business model for those lacking health insurance pioneered by FS gradually became threatened by new legislation. At the beginning of 2003, the government launched the Seguro Popular (universal public health insurance), offering medical coverage to all Mexicans with no formal employment and therefore without access to IMSS or ISSSTE. Seguro Popular coverage grew rapidly, and by 2011 more than 49 million Mexicans were affiliated (43% of the population). As a result, when adding 52 million Social Security system users and users of other public health systems, the country's public health coverage reached over 89% of the population. The market segment of the BoP for FS was therefore reduced from 59% in 1997 to 11% in 2011. As the innovation grew in acceptance, an unforeseen factor came into play: the ability of the system to save service-users time. Although IMSS, ISSSTE, and Seguro Popular are totally free, they have a long waiting list for their services, including emergencies. The BoP population is mostly employed in the informal sector, meaning if people lose time waiting for medical services they lose their daily wage. It is also difficult for employees to obtain permission to visit the doctor's office. BoP clients prefer to spend an average between US$7 and US$10 on a doctor's prescription and medicine than to lose their daily wage waiting in line for free public services.
Despite the increase in public health coverage, the new Pharmacy-Doctor model continued to grow. The perception of poor quality of public health services (such as significant waiting time before being seen by a doctor and a lack of medicine in public health institutions) provided an opportunity for the consolidation of the new model. An interview with a lower middleclass user of state-run medical services revealed that: "even with an advance appointment, the waiting time for a consultation is about three hours." The interviewee further stated that visiting the doctor with no appointment involved an average wait of more than five hours, despite the average consultation not exceeding ten minutes. Finally, the interviewee claimed that "in most cases, four out of five, the drug is not free".
As the Pharmacy-Doctor model started to become more established, positive discussions on the quality of generic medicines and brand-name rights between FS and international drug makers began to take place, resulting in collaboration between the various actors. An example of this would be Sancloz de Mexico, the generic division of the Novartis Group, which began to work towards becoming the supplier for FS. Regardless of the efficiency of implementation and the increasing healthcare coverage resulting from Seguro Popular, the FS Pharmacy-Doctor model continued to grow. The emergence of the model and its nationwide diffusion in the BoP by FS was a huge success.
Imitators in the High-lncome Level Segment
Up until 2011, FS and GI focused on servicing the BoP and had no plans to enter the healthcare field for the middle or upper class in Mexico. In 2009, external events once again affected the dynamics of the model. Mexico was affected by a pandemic (the H1N1 influenza virus), leading to increased regulations of drug sales and making a prescription mandatory for the sale of antibiotics. This became a strong contributing factor to the diffusion of the business model. The treatment of H1N1 was complicated because the Mexican population was accustomed to selfLmedication without the necessity of a prescription. The lack of national regulations preventing the sale of antibiotics without a prescription and the prevalence of self-medication led to the deaths of several people affected by H1N1. In order to address this problem, in May 2010 the government tightened the regulations governing the sale of drugs, particularly the sale of antibiotics. These legislative changes, combined with an ever-increasing time-poor middle and upper classes, helped the Pharmacy-Doctor model to diffuse to large segments of the population.
In 2011, the majority of the national pharmacy chains had adopted the Pharmacy-Doctor model in most of their branches, not just in areas populated by the BoP, but also in mainly middle and upper-class neighborhoods. Initially pharmacies sold brand-name drugs. But by 2011, many adopted the new model, making space within the pharmacy for a doctor's office. Today many pharmacies offer an almost identical model: a physician who can be seen quickly (10 to 15 minutes waiting time) and economically (up to US$2.50 per consultation), attached to a pharmacy offering brand-name (normallypriced) drugs and generic (economically-priced) drugs.
Therefore, the model initially conceived for the BoP in effect migrated upwards to serve middle and upper-income market segments, a process described as trickle-up innovation. Just as with the BoP, the middle and upper classes also go to the pharmacy to consult a doctor in order to treat symptoms not requiring hospitalization. They are able to purchase not only generic drugs, but also brand-name drugs.
The great difference between the BoP and the middle and upper-classes is in the reason why they go to the new Pharmacy-Doctor clinics: the latter group has access to public medical services as well as private insurance (the majority have both) and can easily afford to pay the fees charged by private doctors. The main reason both groups use the service is that they are short on time. Time is extremely valuable for urban populations in general, and the quick service has become the main success factor in the new model. In addition, the requirement for a medical prescription, the proximity of the service to the patient's home and work, and low prices are the main contributory factors behind their decision to use the service.
The middle and upper classes believe that significant time is wasted in waiting to obtain private appointments, and that such appointments, once obtained, are liable to significant delay. In addition, they frequently cost up to US$50 or more. Private health insurance in the country generally has a high deductible, usually more than US$300, and so is not used for common or minor ailments. Pharmacies located in middle or upper-class neighborhoods are spacious, comfortable (with parking and air conditioning) with a large range of medicines and related items. The first pharmacies to offer an onsite medical consultation service, FS, were small stores, with the doctor's office immediately adjacent to the pharmacy, being separated from it by a thin wall. Doctor's offices in Farmacias Guadalajara or Del Ahorro are generally larger in size overall and always have a street-door. In supermarkets such as Walmart the consulting room is usually located inside the store and always next to the pharmacy (see Exhibit 1).
In the beginning, the legislative change making drug prescriptions mandatory negatively affected sales of medicines in drugstores that did not offer low-cost physician consultations. This in turn led to pharmacy chains for all social strata (BoP, middle class, and upper class) seeking to implement the Pharmacy- Doctor business model. As a result, the model diffused upwards socially bringing the Pharmacy-Doctor pairing to middle and upper-class clients. Consumers are willing to pay out-of-pocket for Pharmacy-Doctor clinics to receive care more quickly. Many are willing to use a Pharmacy-Doctor clinic for a minor condition if it means being seen immediately. Pharmacy chains that offer their products to wealthy social classes have thus adopted a model originally designed for the BoP, realizing that there is an opportunity to increase sales due to the fact that even the middle or upper classes do not go to their private doctor for a prescription for minor ailments. As one FS patient commented: "The wait was 10 minutes and the consultation was 15 minutes. The doctor's professional qualification was from a highlyregarded private school in the area. The attention was good and I paid US$1.5 for the consultation and US$2 for the medicine. My eye infection disappeared in two days." Doctors consulting inside the pharmacies also viewed this avenue as a useful way of obtaining experience after graduation and helping them to decide on a future specialization.
Overall, the new Pharmacy-Doctor model is a winwin- win for consumers (patients), drug makers, and doctors. It is a successful innovation that has proliferated throughout the Mexican healthcare industry (Exhibit 2). Looking forward, the Board of Farmacias Similares, which pioneered this model, needs to make a strategic decision: should the firm go international and export the model to focus on the low-income class in other Latin American countries or should it stay domestic and further penetrate the higher-income (middle and upper-class) markets in Mexico.
Appendix 1. The Healthcare Industry in Mexico In 1997 the healthcare industry was mainly made up of the following: the Mexican Public Health Service (IMSS) founded in 1943 and covering 35% of the population; the Government Workers Social Security Scheme (ISSSTE) founded in 1960 and covering 5% of the population; and other social security systems founded between 1940 and 1950 and covering 1% of the population. In 1997, Mexico had approximately 59% of the population without medical coverage, the majority of whom belonging to the BoP. In addition, there is a private network of insurance companies, hospitals, pharmacies, and doctors that charge expensive fees for their medical services and medicines. This private network is used by the middle and upper classes as they can afford to take out private health insurance, and this private network covers 19% of the population. This 19% is already covered by the IMSS or ISSSTE, since these individuals are most likely employees and all employers must provide public service benefits. However, this segment takes out private insurance in order to avail itself of the private network, which is believed to be more efficient than the IMSS or ISSSTE: only in extreme cases does this segment use the public service. The individuals who comprise of the BoP, who are excluded from public medical services and unable to afford the private services, generally have to use alternative medicines, such as homeopathy, herbal medicine, and traditional healers that arc the only options economically available to them.
The network of private pharmacies sells only brandname drugs manufactured by international drug makers, while public-sector pharmacies use mainly generic drugs manufactured by national and international drug makers. Since the IMSS has the widest population coverage, competition among companies to be official suppliers has resulted in allegations of widespread corruption. Another noteworthy characteristic of the medical industry is the excellent social status that doctors have, along with the excellent wages they can earn in private hospitals or consultancies. Annually more doctors graduate from Mexican universities than are required in large urban areas. There is a scarcity of doctors in rural areas, but the majority prefer urban to rural environments as low-income people are often unable to pay for medical services. As a result, many medical graduates swell the ranks of the urban underemployed, filling temporary positions. This is a general picture of the conditions prevailing in the medical
industry in Mexico in 1997.
1) © Miguel A. Montoya and Mauricio Cervantes. Reprinted with permission.
2) Generic medications are those sold under the name of the active ingredient, in contrast to brand-name drugs that are manufactured worldwide by different pharmaceutical companies for brand-name owners.
Sources: Extracted from (1) company web pages; (2) Euromonitor International, 2012, Consumer Health-Mexico, Retrieved February 12, 2012, www.euromonitor.com/mexico; (3) R Keckley, S. Coughlin, L. Korenda, G. Moreno, 2011, Survey of Health Care Consumers in Mexico: Key Findings, Strategic Implications, Deloitte Center for Health Solutions.
Exhibit 1 Examples of Pharmacy-Doctor Model Layouts
Exhibit 2 Growth of the pharmacy-Doctor Model in the Base of the Pyramid in Mexico, 1997-2011
Number of pharmacies of FS and GI combined.
From a resource-based view, how easy or difficult it is for competitors to offer a similar Pharmacy- Doctor business model? Given your answer, how sustainable is FS's competitive advantage?
Explanation Verified
Verified
Sustainability of FS with a new pharmacy...
Global Business 4th Edition by Mike Peng
Why don’t you like this exercise?
Other Minimum 8 character and maximum 255 character
Character 255



